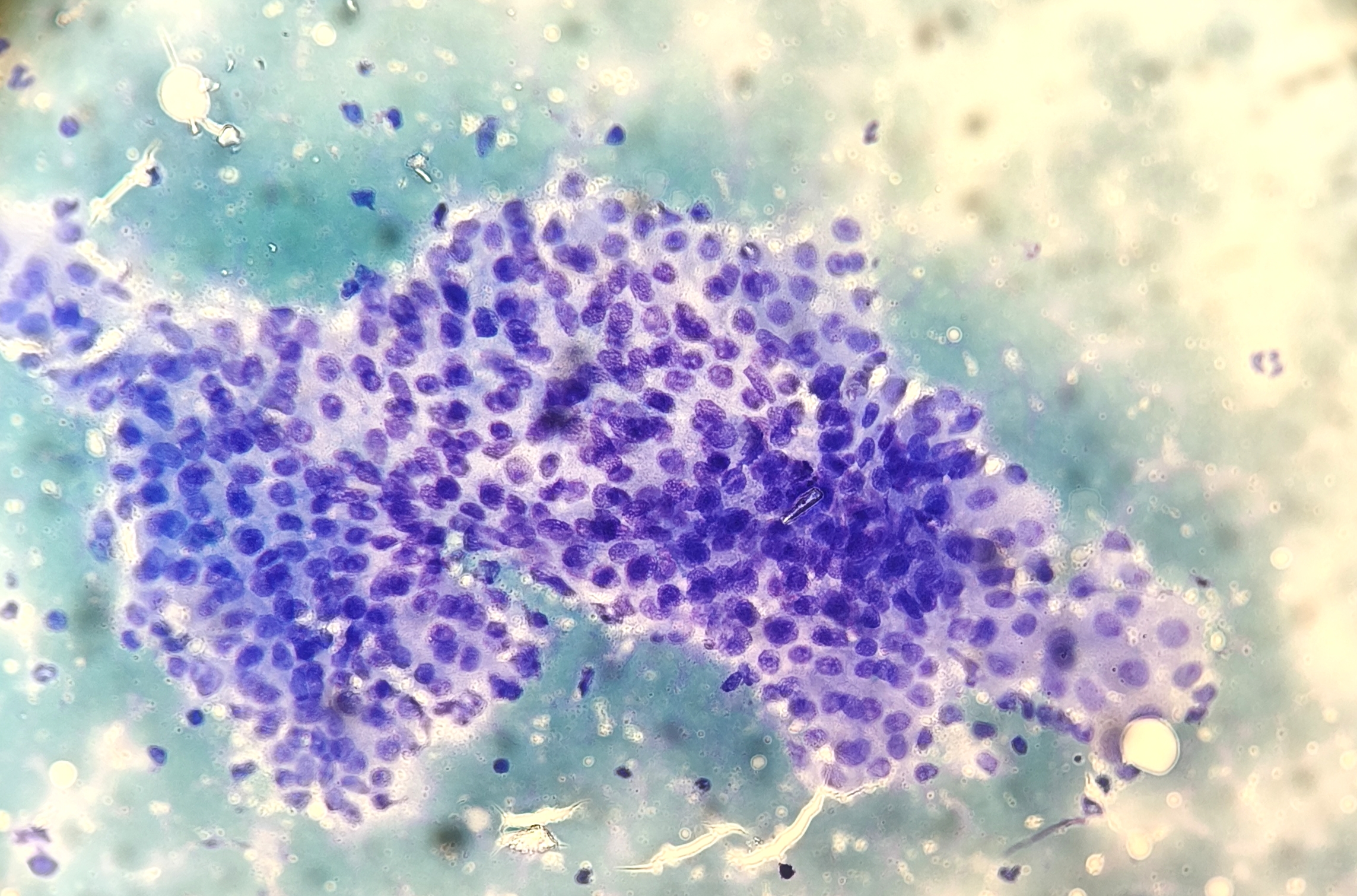
An 80-year-old male patient presented with a hypoechoic, nodular lesion of approximately 21 mm in the right parotid gland. Clinical suspicion was of a pleomorphic adenoma. Cytopathologic assessment via fine needle aspiration (FNA) was performed.
Editorial Note: In our initial publication, we unintentionally failed to mention current president Carme Dinarés and her contributions to the Spanish Society of Cytopathology. Please see the extended article with an additional section acknowledging her role and achievements.
The Spanish Society of Cytopathology (Sociedad Española de Citopatología)
The Spanish Society of Cytopathology (Sociedad Española de Citopatología, or SEC) is an organization dedicated to studying, practicing, and advancing cytopathology in Spain. The SEC plays a vital role in ensuring high standards of practice and focuses primarily on fostering professional development and promoting research in the area of cytopathology. Furthermore, it creates a network among cytology practitioners that allows better case consultation, training and guidance from renowned mentors. The SEC was officially founded in 1988 with the purpose of fulfilling the need for a formal organization that could represent professionals working in the field of cytopathology. Before the formation of SEC, Spanish cytopathologists worked in a fragmented manner. Since then, the increasing importance of cytological techniques in diagnostic medicine, the need for a specialized organization became more apparent and the society has tried to meet the demands of its members. Since its inception, the society has played an instrumental role in advancing cytopathology as a discipline, supporting its members, and improving diagnostic practices in Spain. Furthermore, SEC is an active member of several international organizations, such as the European Society of Cytopathology (ESC) and the International Academy of Cytology (IAC). These collaborations allow the SEC to contribute to and benefit from global initiatives in the field. Membership of the Spanish Society of Cytopathology consists of professionals working in the field of cytopathology, including pathologists, cytotechnologists, laboratory technicians, and researchers. Membership is open to individuals working in Spain and internationally. Members benefit from various services and opportunities offered by the SEC. These include access to professional development programs, scientific meetings, and an array of educational resources. The SEC organizes a national scientific meeting every other year. In addition, the SEC offers its members interactive courses throughout the year. Such as monthly lectures given on crucial topics and aimed at pathologists, oncologists, molecular biologists and cytotechnicians; or offering monthly challenging cases. The governance of the Spanish Society of Cytopathology is managed by an elected board, which is responsible for overseeing the organization’s operations, setting its priorities, and guiding the society’s activities. The board includes a president, vice president, secretary, treasurer, and one representative from the society. These positions are elected for two years, with the former president playing a crucial role as an advisor to the new board. In this way, society can maintain a certain continuity thatenables long-term planning, from which all members benefit. On the other hand, since Spain is a large country, a regional representative is appointed for each region to ensure closer proximity to the board and its members. For the past two years, the society has been led by Carme Dinarés. During her presidency, the SEC organized its biennial congress in September 2024 in the city of Gijón, Asturias. In addition to this congress, she has promoted two interactive courses. The first, “Cito-Tour,” is a monthly lecture series where pathologists, oncologists, molecular biologists, and cytotechnicians come together to discuss key aspects of tumors and the role of cytopathology in diagnosis and treatment. The second, “What is Your Cytological Interpretation?”, is an online course designed for pathologists, cytopathologists, anatomical pathology technicians, and cytotechnologists. This course presents a monthly case selected for its clinical relevance, diagnostic challenges, and educational value where participants can refine their diagnostic skills and expand their knowledge. She has also promoted international academic alliances with SLAC (Latin American Society of Cytology). Furthermore, during her presidency, the SEC has been accredited with the ISO 17043 standard. As a result of years of work of the different boards chaired by doctors Charo Granados, Belen Lloveras and Lola Lozano, ENAC has finally granted them accreditation (19/PPIO26) for the quality control of Q-Pap and molecular Q-Pap. This is a very important achievement, which means that the SEC is currently the only European scientific cytology society accredited to carry out intercomparison exercises of adjusted cervical cancer screening programs. The SEC believes that this achievement will undoubtedly contribute to improving the quality of cervical cancer screening diagnoses, which is why it wants to offer all professionals this quality control in order to improve our diagnosis in this field. The society has amongst its members professionals with recognized international presence. Such is the case of the former president, María D. Lozano, better known as Lola by many. Her expertise in the field and worldwide recognition has enabled the SEC to gain visibility nationally and internationally. Her presidency has allowed its members to connect with some of the most prestigious cytopathologists across Europe, the United States of America, and Latin America. Some examples of the visibility Dr. Lozano gave to the SEC during her presidency could be the ASC-SEC course in Pamplona 2020 and a scientific reunion in Granada, Spain, in September 2022, with the participation of Syed Z. Ali, Merce Jorda, Philippe Vielh, Peter B. Illei, and Paul E. Wakely, among others. Her journey continues as she prepares to become the president of the Spanish Society of Pathology (SEAP) and the Spanish division of the Internal Academy of Pathology. In this role, she aims to replicate the successes of the SEC and strengthen the connections between both organizations, emphasizing the importance of cytologic and surgical pathology correlation for improved patient care. To conclude, the Spanish Society of Cytopathology plays a central role in advancing education, research, and clinical practice in this specialized field. Through its active programs, educational initiatives, and collaborative efforts with international organizations, the SEC ensures that its members remain at the forefront of diagnostic advancements that benefit patients. Furthermore, in the coming years, with thecooperation between SEC and SEAP-IAP, cytopathology and surgical pathology in Spain are set to work side by side to place patients at the center of all our efforts.
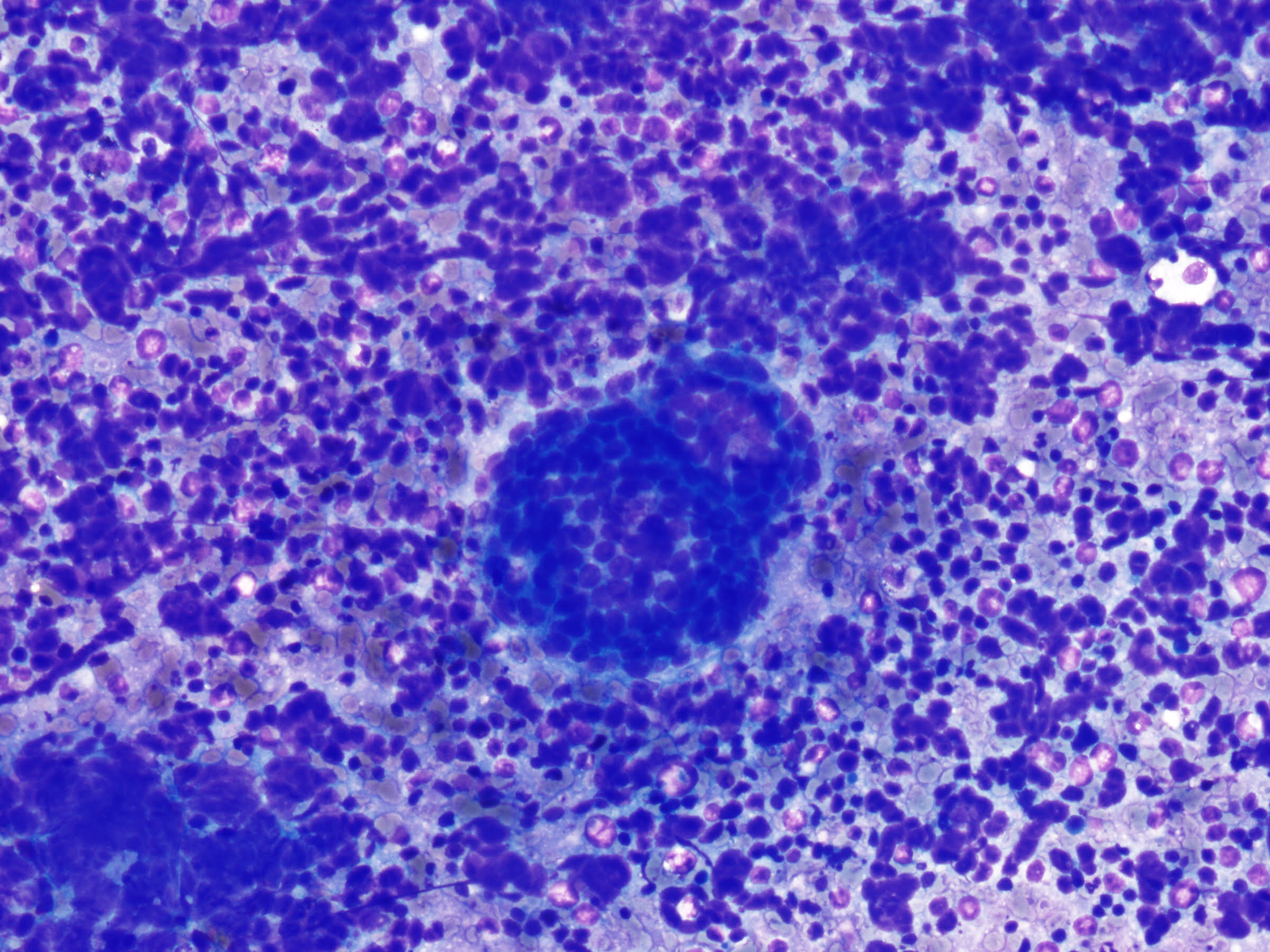
COMBINED SMALL CELL CARCINOMA AND ADENOCARCINOMA DIAGNOSED ON EBUS-TBNA MATERIAL
Author: Cisel Aydin Mericoz MD, Pinar Firat MD, Institution: Koç University Hospital, Department of Pathology, İstanbul, Türkiye
CLINICAL PRESENTATION:
A 64-year-old male patient presented with a 2.5-month history of numbness and severe pain in the arms and legs. He was initially treated with physical therapy, without clinical improvement. A thoracic CT scan revealed a 2 cm, well-circumscribed lesion in the left upper lobe and extensive mediastinal lymphadenopathy, including the left hilar region. EBUS-guided transbronchial needle aspiration (EBUS-TBNA) was performed for diagnostic purposes.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies. Cookies Policy
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.